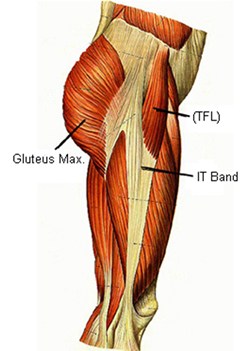
IT Band Friction Syndrome is a common repetitive strain injury of the lateral knee. The IT Band can become inflamed and irritated, when it is pulled over the lateral condyle of the knee. This is common in cyclists, as the thousands of repetitions cause a repetitive strain. Stretching the IT Band can reduce the amount of tension on the tissue, as it moves over the.knee. This in combination with rest, is all that is generally needed to resolve this condition.
This condition is common with people who are experiencing Patellofemoral Syndrome.

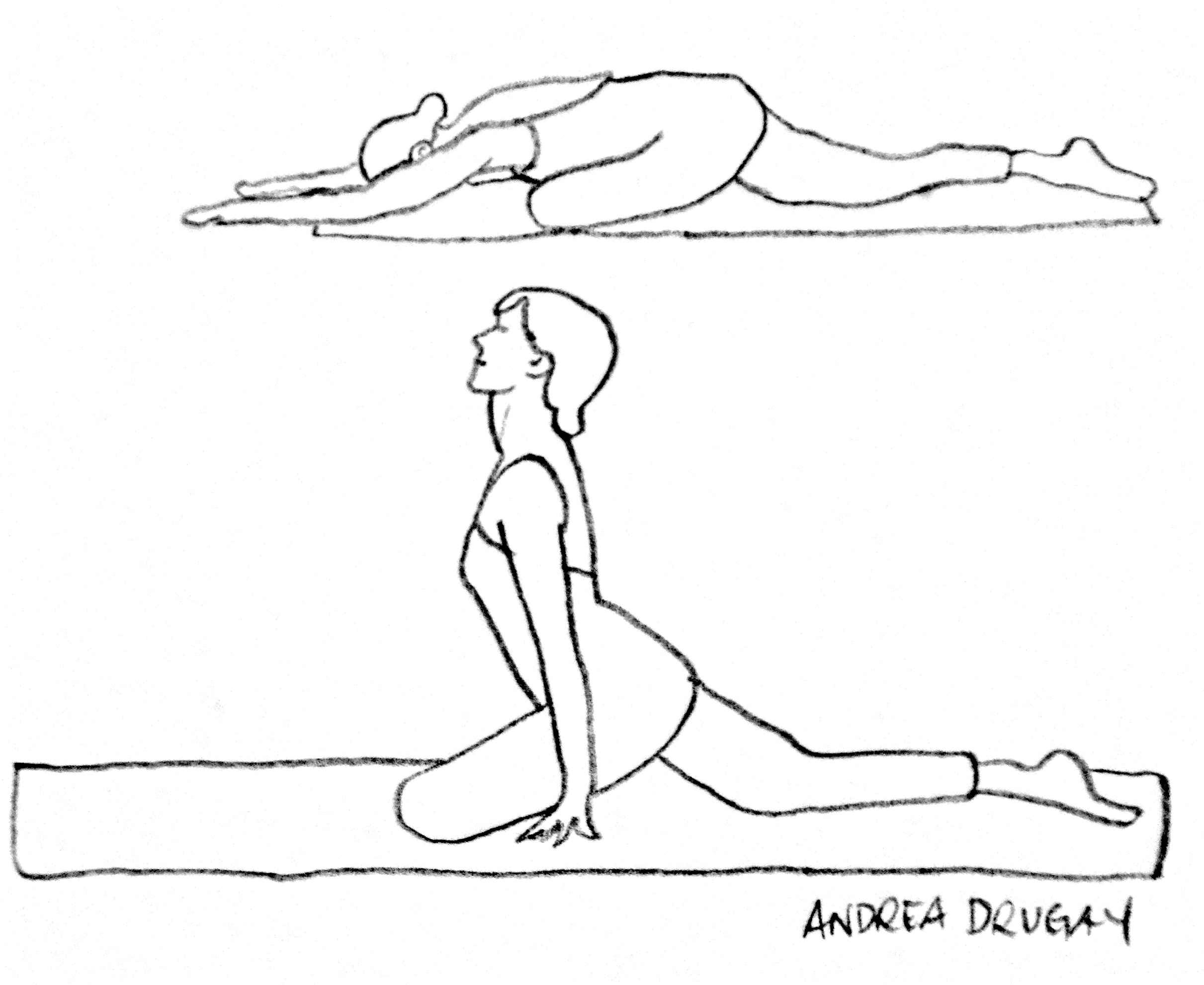
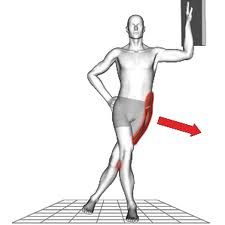
Stretching




Orthopedic Test
Ober’s Test
Assessing For: the length of the Iliotibial band and Tensor Fascia Lata
Procedure:
- Patient is sidelying close to the edge of the table on the unaffected leg. Therapist stands behind the Patient.
- Flex hip and knee of the unaffected leg that is at the bottom
- Stabilize the Patient’s pelvis with one hand
- With the other hand grasping the medial aspect of the patient’s affected knee, passively hyperabduct and extend the affected femur at the hip.
- Allow the affected leg to lower without rotating
Positive Sign: the affected leg stays abducted and does not lower.
Noble’s Test
Testing for:
The presence of iliotibial band (ITB) friction syndrome
Procedure:
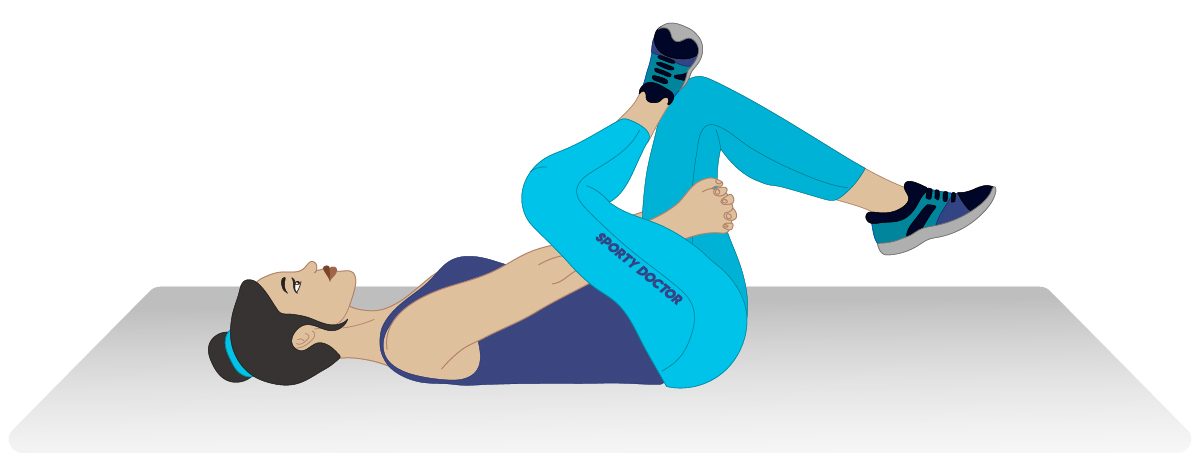
- Patient is supine, with both their affected side’s knee and hip flexed to 90° degrees
- Therapist compresses the iliotibial band (ITB) – 2 centimetres proximal to the lateral femoral condyle
- Instruct the patient to extend the knee and hip slowly while therapist maintains compression of the ITB proximal to the lateral femoral condyle
Positive Sign:
Pain over the lateral femoral condyle at about 30° degrees of knee extension
Minor Effusion Test (aka Brush Test)
Purpose:
To assess for lesser amounts of synovial fluid within the knee joint right after an injury. This is usually done after the Major Effusion Test comes up negative.
Procedure:
- Patient is supine, their affected knee is extended as much as they can
- Therapist slowly sweeps the effusion from the superior lateral aspect of the knee and suprapatellar pouch
Positive Sign:
A bulge inferior to the patella appears within two seconds, the positive test will indicate from 4-8 millimeters of extra synovial fluid within the joint. This could be caused by cruciate or meniscal damage and is considered a Medical emergency.
Valgus Stress Test of the Knee
Testing for:
The integrity of the structures that prevent Valgus deformity of the knee (Joint capsule, medial collateral ligament, cruciate ligaments)
Procedure:
- Patient is supine
- Place the affected leg in extension and slight external rotation.
- Stabilize with one hand on the medial malleolus and with the other hand stabilize the lateral aspect of the knee
- Apply a medially directed stress on the lateral knee
- Flex their knee to 30 degrees and apply the same pressure on the lateral side to isolate the medial collateral ligament
Positive Sign:
Presence of pain and hypermobility at the medial aspect of the knee
Special Test Physical therapy
Varus Stress Test of the Knee
Testing For:
The integrity of the structures that prevent lateral instability at the knee (lateral collateral ligament, joint capsule, cruciate ligaments).
Procedure:
- Patient is supine with the affected knee in full extension.
- Therapist stabilizes the affected leg in slight external rotation with one hand on the lateral malleolus.
- Therapist places their other hand on the medial aspect of the knee.
- Therapist applies a laterally directed (a varus) stress on the medial knee.
- Flex their knee to 30 degrees and apply the same pressure on the lateral side to isolate the lateral collateral ligament
Positive Sign:
Presence of pain and hypermobility at the lateral aspect of the knee
Lachman’s Test
Testing for :
The integrity of the Anterior Cruciate Ligament (ACL). The Lachman’s test is considered to be the most accurate test for ACL integrity.
Procedure 1:
- Patient is supine
- Patient’s affected knee is flexed 30°
- Therapist stabilizes distal femur with one hand while grasping patient’s proximal tibia with the other hand
- Therapist applies an anteriorly directed stress the tibia.
Procedure 2:
- Patient is seated with their affected leg over the edge of the table
- Therapist sits in front of the patient, supporting the patient’s ankle on therapist’s thigh
- Therapist places patient’s knee in 30° flexion
- Therapist stabilizes the distal femur with one hand
- Therapist applies anteriorly directed stress on the proximal tibia with the other hand
Positive Sign:
Pain or excessive anterior motion of the tibia, and disappearance of the infrapatellar tendon slope.
Patellar Apprehension Test
Purpose:
To test whether the patella is likely to dislocate laterally
Procedure:
- Patient is supine with their affected knee extended
- Therapists uses a slow and moderate pressure against the medial aspect of the patella moving it in a lateral direction
- Therapist observes patient’s reaction
Positive Sign:
Patient expresses apprehension and/ or might try to move their affected knee away from the pressure.
Helfet’s Test
Testing for:
The dynamic rotary function of the Tibia (possible torn meniscus or injured cruciate ligament)
Procedure:
- Patient is seated, with their legs hanging over the edge of the table
- Patient’s knees flexed to 90° (so the tibial tuberosity is perpendicular to the midline of the patella)
- Therapist slowly extend the patient’s knee
- As the knee is slowly extended, the Therapist observes the relative alignment of the tibial tuberosity to the midline of the patella.
- (Therapist can also palpate the movement of the tibial tuberosity).
* Since the medial femoral condyle is about 1 cm. longer than the lateral femoral condyle, the tibia first moves over the available lateral condyle surface and then must rotate laterally when we extend the knee.
* it’s impossible to perform helfet’s test if there is knee joint effusion
Positive Sign:
Absense of slight lateral tibial motion = this positive sign may indicate that a torn meniscus or injured cruciate ligament is physically blocking the knee extension.
