Description
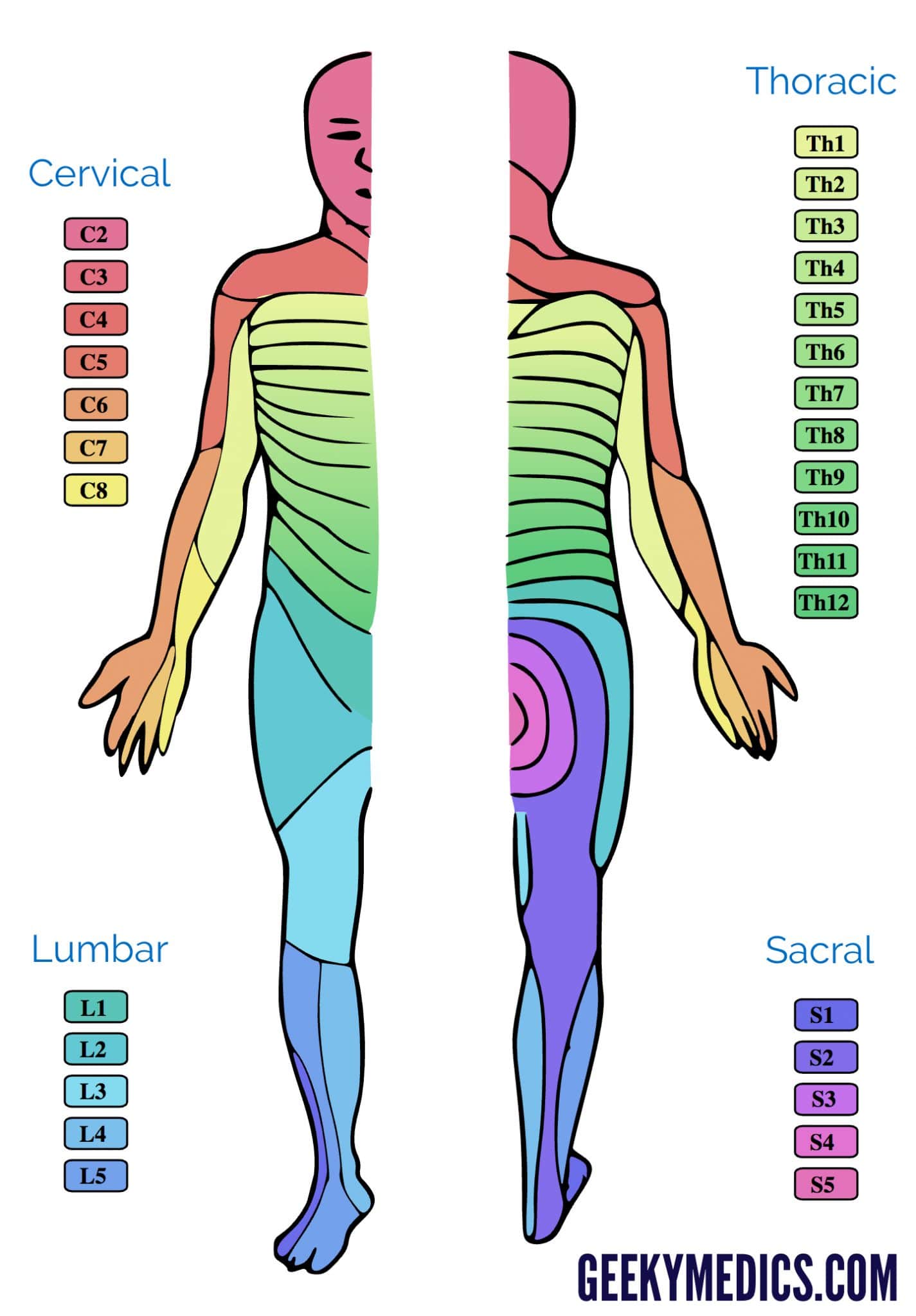
Thoracic outlet syndrome (TOS) is a term used to describe a group of disorders that occur when there is compression, injury, or irritation of the nerves and/or blood vessels (arteries and veins) in the lower neck and upper chest area.
TOS can be caused by tight Scalene or Pectoral muscles (among others). By stretching and massaging these muscles, we can reduce the amount of stress these muscles put on the affected nerve.



Stretching and Self-Massage



Orthopedic Tests
Adson’s test involves asking the client to rotate the neck ipsilaterally, flex it laterally to the opposite side, and extend the neck at the spinal joints (the opposite actions of the actions of the anterior and middle scalenes), while the therapist is palpating the radial pulse
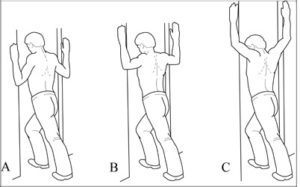
Eden’s test for costoclavicular syndrome form of thoracic outlet syndrome. The client is asked to push the chest out and pull the shoulders back as if standing at military attention, while the therapist palpates the strength of the radial pulse. (Courtesy Joseph E. Muscolino.
Halstead ttest. The patient is sitting or standing. The therapist continuously palpates the radial pulse on the side being tested. While still palpating the radial pulse, the therapist abducts the arm to 45 degrees, extends the shoulder to 45 degrees, and externally rotates the upper extremity while applying a downward distraction to the arm. The patient is then asked to fully turn her head away from the side being tested and extend the cervical spine.
Spurling’s Test. The patient is seated and asked to sidebend and slightly rotate head to the painful side.The therapist places a compressive force of approximately 7 kg through the top of the head in an effort to further narrow the intervertebral foramen.The test is considered positive when it reproduces the patient’s symptoms. The test is not indicated if the patient does not have upper extremity or scapular region symptoms.
Anterior Neck Flexors Strength Test
Purpose:
To asses the strength of the neck flexors (SCM, anterior scalene, supra and infrahyoids, longus colli and capitis, and rectus capitis anterior)
Procedure:
- Patient is supine
- Patient abducts arm to 90°, flexes the elbows to 90°, and rest their dorsal hands on the table.
- Patient tucks chin, and then lifts head off the table.
- Patient keeps the head lifted off the table (Grade 3). Patient resists therapist posteriorly-directed pressure (Grade 5)
Positive Sign:
Weakness of Anterior Neck Flexors if Patient is unable to keep the neck in flexion against gravity or the therapist’s pressure.
Anterolateral Neck Flexors Strength Test
Purpose:
To asses the strength of the Anterolateral Neck Flexors (SCM and scalene on one side).
Procedure:
- Patient is supine
- Patient abducts arm to 90°, flexes the elbows to 90°, and rest their dorsal hands on the table.
- Patient rotates the head away from the side being tested. Therapist stabilizes the side being tested.
- Patient lifts the head into slight flexion and hold it against gravity.
- Patient keeps the head lifted off the table (Grade 3).
- Therapist holds the temporal region on the side being tested.
- Therapist pushes in an oblique posterolateral direction, away from the tested side.
Positive Sign:
Weakness of the Anterolateral Neck Flexors if the patient is unable to keep the neck in flexion against gravity or the therapist’s pressure.
Cervical Compression Test
(for patients who cannot rotate or extend their head)
Testing For:
Compression of cervical nerve root or facet joint irritation in the Lower Cervical Spine
Procedure:
- Patient is seated.
- Patient’s head is in neutral.
- Therapist stands behind patient.
- Carefully apply compression downward on the head of the patient.
Positive Sign:
Radiating pain or other neurological signs in the same side arm (nerve root) and/ or pain local to the neck or shoulder (facet joint irritation).
Cervical Distraction
Purpose:
To relieve the pressure on the cervical nerve roots (may be used after Spurling’s or Cervical Compression Tests)
Procedure:
- Patient is supine or seated. Patient’s head is in a neutral position at all times throughout the procedure.
- Therapist grasps the patient’s head at occiput and temporalis. One hand on either side of the head.
- Slowly traction the patient’s head in a superior direction. Maintain the traction for at least 30 seconds.
First Rib Mobility Test
Purpose:
To test the mobility of Rib 1
Procedure:
- Patient is seated.
- Patient fully rotates their head away from the side being tested.
- Patient then fully flexes the head to their chest.
Positive Sign:
Patient has limited neck flexion. The cause for the hypomobilty may be tight scalenes
Related
Mytones